
From the 1Merem Medical Rehabilitation, Hilversum, 2Amsterdam UMC, University of Amsterdam, Department of Rehabilitation, Amsterdam Movement Sciences, Meibergdreef 9, Amsterdam, 3Saxion University of Applied Sciences, Research Group Mechatronics, Enschede, and 4Donders Centre for Brain, Cognition and Behaviour, Radboud University Medical Centre, Department of Rehabilitation, Nijmegen, The Netherlands
Objective: To determine the concurrent validity and reliability of a low-cost spatiotemporal gait analysis system for clinical use in rehabilitation medicine.
Design: Cross-sectional study.
Subjects: Thirty-three healthy adults.
Methods: The spatiotemporal gait analysis system consists of a video camera placed perpendicular to a 10-m walkway and calibrated for spatial reference. The conditions evaluated in this study were: barefoot walking at comfortable and slow speed, toe and shod walking using a stationary camera setup and barefoot walking at comfortable speed using a moving camera setup. The GAITRite® was used as reference.
Results: High intraclass correlation coefficients (ICC≥ 0.97; 95% lower limit confidence intervals (95% CIs) ≥ 0.77) were found between systems for step and stride length, and step, stance and stride time, across setups and conditions. Standard error of measurement and Bland-Altman repeatability coefficients were ≤ 2.4% and ≤ 6.3%, respectively. A minimum of 4 footsteps was required to obtain ICC >0.90 and coefficient of variation < 10%. For double support and swing time, ICCs were generally low (ICC≥ 0.21). Inter-rater reliability was excellent for step length, step and stance time (ICC≥ 0.94; lower limit 95% CIs ≥ 0.86).
Conclusion: The spatiotemporal gait analysis system is valid and reliable for assessing spatiotemporal parameters in different walking conditions. However, the validity of double support and swing time could not be confirmed.
Key words: spatio-temporal analysis; gait; video recording; motion capture; reproducibility of results.
Accepted Apr 25, 2019; Epub ahead of print May 10, 2019
J Rehabil Med 2019; 00: 00–00
Correspondence address: Maijke van Bloemendaal, Merem Medical Rehabilitation, Soestdijkerstraatweg 129, NL-1213 VX Hilversum, The Netherlands. E-mail: mbloemendaal@merem.nl
Gait parameters, such as step length and step time, allow the quantification of gait deviations in persons with various diseases. Treatment can be customized and evaluated based on these parameters. However, few low-cost, easily applicable systems are available for clinical settings to accurately measure gait parameters. A low-cost spatiotemporal gait analysis system was developed and this study evaluated its accuracy and reliability. The spatiotemporal gait analysis system consists of a camera placed perpendicular to the walkway, which can be used stationary or moved manually along a parallel rail system to capture multiple strides of an individual during a single walk. Thirty-three healthy adults completed trials of barefoot, toe and shod walking. These adults were simultaneously recorded using an electronic walkway, the GAITRite®, for comparison. The results showed that the spatiotemporal gait analysis system is an accurate and reliable system to assess step and stride length, step, stance, and stride time, but not to assess double support and swing time.
Gait deviations are among the most commonly reported impairments in persons with a variety of neurological and musculoskeletal conditions (1–7). Evaluation of the effectiveness of interventions targeting gait requires sensitive and objective assessment of gait characteristics (8). Gait speed is the outcome most often used in clinical practice, and commonly assessed with timed walking tests, such as the 10-m and 6-min walk test, using a designated track and stopwatch. However, these methods are limited for assessing other spatial and temporal parameters that are considered important to properly evaluate gait, such as step length and step time and derivative parameters such as gait symmetry (8–11). The validity of simple measurement methods, such as the stopwatch-footfall count method to assess step length, has not been confirmed (12). Clinical evaluation of these spatiotemporal characteristics is essential for identifying and understanding gait deviations, guiding clinical decision-making, customizing treatment, monitoring individual progress, and proving treatment benefits (1–6).
Valid and reliable systems assessing spatiotemporal gait parameters include 3-dimensional motion capture systems, and electronic walkways, such as the GAITRite® system (13–18). However, these systems are relatively costly and, regarding the 3-dimensional systems, too sophisticated for measuring spatiotemporal variables in a clinical setting. In case of electronic walkways, there may be practical issues, such as with restricting the subjects to walk within the relatively narrow width of the carpet and requiring them to walk on and off the carpet (19). Several low-cost systems exist that use a single-camera setup, footswitches, accelerometers, gyroscopes, and inertial measurement units; however, results on the accuracy of spatial parameters are inconsistent or absent and it is questionable whether some of these systems are reliable in persons with gait deviations (e.g. forefoot contact at initial contact) (19–30).
A 2-dimensional spatiotemporal gait analysis system (SGAS) at relatively low-cost (approximately one-tenth of the price of a GAITRite® system) was developed that measures spatiotemporal gait parameters in the sagittal plane using a single camera placed perpendicular to the walkway. The camera can either be used in a stationary position, or moved manually along a parallel rail system to capture multiple strides during a single walk. The SGAS uses custom software for camera calibration and position and time measurement (31). Individuals walk unobtrusively while their gait is recorded with the camera. To our knowledge no camera system using this calibration method has been validated for assessing spatiotemporal gait parameters.
The aim of this study was to establish the concurrent validity of the SGAS for assessing the spatiotemporal parameters of gait in healthy subjects under 4 different walking conditions: barefoot walking, shod walking, and to mimic gait deviations that may result from neurological or musculoskeletal disorders, toe walking and slow walking. Furthermore, the minimum number of footsteps needed to achieve reliable estimates of spatiotemporal gait parameters, inter-rater and intra-rater reliability, and measurement error were determined.
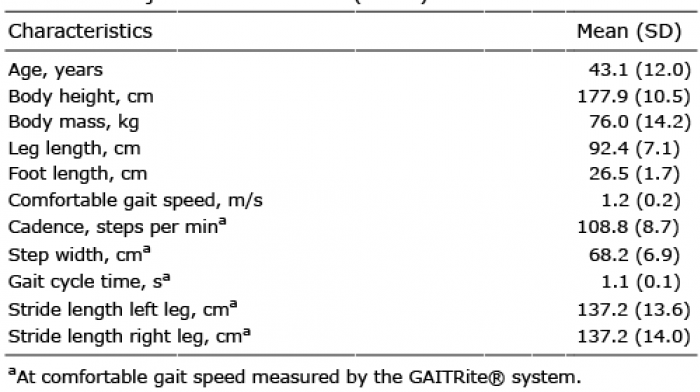
A sample of 33 healthy adults (13 men, 20 women, mean age 43 years, standard deviation (SD) 12 years) were recruited from employees, their relatives, and visitors to our rehabilitation centre through flyers posted at the centre (see Table I for subject characteristics). Individuals were eligible if they were over 18 years of age, could walk independently, and were free of musculoskeletal or neurological pathology. Data collection took place at the human movement laboratory of our centre. The study protocol was approved by the medical ethics committee of the Academic Medical Centre of the Amsterdam University Medical Centres (protocol number NL50002.018.14). All subjects provided written informed consent.
Table I. Subject characteristics (n=33)
The SGAS consists of a high-definition 2.2-megapixel camera with 50× optical zoom (f/1.8–4.2, 16:9), sampling at 50 Hz (Panasonic Corporation, Osaka, Japan). Custom software on a Windows computer with a high-definition multimedia interface (HDMI) frame grabber was used for camera calibration, video recording, and position and time assessment (TMSi, Oldenzaal, The Netherlands). The SGAS software is available open source (https://github.com/MvanBloemendaal/SGAS). The camera was levelled and positioned on a movable tripod (camera dolly). In this study, the camera was positioned at a height of 92 cm and the perpendicular distance from a 10-m long walkway equals 360 cm (schematic representation in Fig. S11). The camera was used both in a stationary position (a length of 130 cm of the walkway could be captured reliably within the field of view) and as a moving camera on a 7-m long rail (dolly track) placed parallel to the walkway, over which the camera could be moved manually (Fig. 1). An overview of the SGAS requirements and costs is presented in Appendix S11.
Fig. 1. Spatiotemporal gait analysis system (SGAS): camera positioned on a movable tripod and the computer screen with the software.
The SGAS measures calibrated positions on the floor of the walkway. The calibration procedure is based on the method proposed by Zhang (31). Intrinsic camera parameters are determined from approximately 30 images of a planar 6×10 chequerboard pattern of 9-cm squares (Fig. 2). These parameters characterize the camera’s optical system. Placing this chequerboard pattern vertically in a well-defined location on the walkway sets up an orthogonal laboratory coordinate system in which the y-axis runs along the walkway, the x-axis is perpendicular to the walkway, and the z-axis points vertically upwards. The position and orientation of the camera with respect to this coordinate system are determined from a single image of the chequerboard pattern at this location. This image provides the information for the camera’s extrinsic parameters. Combining the intrinsic and extrinsic parameters results in the camera’s projection matrix, which describes how the coordinates of a point in the laboratory coordinate system are converted into the pixel coordinates of the camera’s image plane. In the current study, the set-up and calibration process of the SGAS took approximately 10 min; calibration was repeated after assessing 8 subjects and in a clinical setting requires one calibration for the day.
Fig. 2. Calibration of the camera for determining the projection matrix.
The y-coordinates of an object on the floor are determined manually from the video image. On the basis of the projection matrix, the SGAS software draws a thin red line in the video image representing the projection of the line in the x-direction for a given y-coordinate in the plane z = 0 (Fig. 3). The user adjusts the y-coordinate of this line by moving the computer’s mouse until the projection matches the position of the object on the floor in the image; for instance, the location of heel contact of a foot. The user reads the corresponding y-coordinate from the SGAS user interface. The time of the event is derived from the video frame rate (time resolution 0.02 s). Counting the number of frames yields the time difference between 2 events in the video recording.
Fig. 3. Video analysis using the spatiotemporal gait analysis system (SGAS).
Simultaneously with the SGAS, the gait of the subject was recorded with the GAITRite® system. The GAITRite® system (GAITRite® Platinum 488P, CIR Systems Inc., New York, USA) consists of a portable carpet walkway embedded with pressure-activated sensors that sample at 60 Hz. The walkway is 488 cm long and 61 cm wide and contains an active sensor area of 384 × 48 sensors arranged 1.27 cm from each other (centre on centre, 18,432 sensors in total).
During a 30-min test session, subjects were tested in 4 different walking conditions in a fixed order under stationary camera set-up: barefoot walking at comfortable speed; barefoot walking at slow speed; barefoot toe walking at comfortable speed; and shod walking at comfortable speed wearing their own comfortable flat-soled shoes. Data collection with the SGAS and GAITRite® system was conducted by one investigator (MVB).
Ten valid gait trials, 5 in which a left and 5 in which a right footstep was visible within the 130-cm field of view, per walking condition were collected with the GAITRite® system and SGAS in a stationary position. Gait strides were collected in the given field of view by the stationary SGAS camera for the conditions of slow speed and toe walking.
In addition to the stationary camera conditions, while walking barefoot at a comfortable walking speed, 4 gait trials, including 4–8 strides per trial, were collected with the SGAS camera being moved along the walkway by the investigator.
Inter-rater reliability was assessed with 3 trained observers who were instructed in the definitions of the spatiotemporal gait parameters (Table SI1) and gait analysis method. To assess intra-rater reliability, one observer (MVB) assessed the same data on 2 different occasions (minimally 1 month apart). Inter-rater and intra-rater reliability were assessed for the barefoot comfortable walking condition with the stationary SGAS camera.
The initial contact (heel or toe) and toe-off distance and time-points during each trial were identified manually from the video images of the SGAS by 5 trained observers and were recorded in a Microsoft Excel spreadsheet format (Microsoft Corporation, Washington, USA) that was designed to automatically calculate the spatiotemporal gait parameters (https://github.com/MvanBloemendaal/SGAS). Analysed data from the SGAS and the GAITRite® system were: step length, step time, stance time, double support time, stride length, stride time, and swing time.
Concurrent validity was evaluated from the intraclass correlation coefficients model 2,1 (ICCs2,1) using a 95% confidence interval (95% CI), and the standard error of measurement (SEM) and percentages (%SEM) were calculated from an analysis of variance. The SEM was considered small if it represented less than 5% of the weighted mean. Systematic differences between the systems were determined using paired t-tests. Based on the resolution of the GAITRite® system for spatial (1.27 cm) and temporal (0.02 s) parameters, differences smaller than these values were considered as measurement error. Bland-Altman repeatability coefficients (RCs) were calculated as 1.96 times the standard deviation of the difference between the 2 systems under comparison. The RC was considered small if it represented less than 8% of the weighted mean, which was the RC found between the GAITRite® system and 3-dimensional gait analysis systems (32).
To determine the minimum number of footsteps needed to achieve an adequate level of reliability for the SGAS data, ICCs model 3,1 (ICCs3,1) were calculated per gait parameter for 2 steps and for each incremental step (n) up to 10 steps. Subsequently, a coefficient of variation (CoV) was calculated between the 95% limits of agreement interval (calculated as the mean difference of n steps and 10 steps ± 1.96 times the SD of the difference between n steps and 10 steps) divided by the mean value for 10 steps. Data were considered reliable when this CoV was < 10%. Inter-rater and intra-rater reliability were examined using ICCs (inter-rater: ICC2,1 and intra-rater: ICC3,1) with 95% CIs.
The following classification for the ICC was used: poor (< 0.50), moderate (0.50–0.74), good (0.75–0.89), and excellent (≥ 0.90). An ICC with a value of 0.90 or greater and a lower limit of the 95% CI of at least 0.75 were considered as acceptable (33). For all ICCs, the absolute agreement criterion was used. The presence of heteroscedasticity was examined through visual inspection of the Bland-Altman plots. To ensure statistical power, a sample size of at least 30 subjects was required (34). Significance was set at p < 0.05. Data analysis was performed using IBM SPSS Statistics 23.0 (SPSS Inc., Chicago, IL, USA).
Approximately 78–98% of the collected data across walking conditions for the stationary and moving setup of the SGAS and the GAITRite® system was applicable. Most missing data came from invalid trials with the GAITRite® system due to steps outside the active sensor area and errors in the foot detection of the sensors. In total, between 256 and 322 valid trials of footsteps across conditions for the stationary and moving setup were collected from the SGAS and
GAITRite® data (Table II). In addition, data were collected for between 150 and 256 valid trials of strides across conditions for the moving setup and for the conditions slow gait speed and toe walking from the stationary setup of the SGAS and the GAITRite® system.
Table II. Concurrent validity and measurement error between the spatiotemporal gait analysis system (SGAS) and GAITRite® system for all conditions for 10 footsteps per subject
Excellent agreement for step length, step time, stance time, swing time, stride length, and stride time was found between the SGAS and the GAITRite® system in all walking conditions (ICC ≥ 0.95 and lower limit of the 95% CIs ≥ 0.78; Table II). Double support time showed poor agreement for the condition comfortable gait speed (ICC = 0.21 and lower limit of the 95% CI = 0.02), moderate agreement for the condition toe walking (ICC = 0.50 and lower limit of the 95% CI = –0.06), and good agreement for the conditions of shod walking and slow gait speed (ICC ≤ 0.83 and lower limit of the 95% CIs ≤ 0.75, Table II). Moreover, systematic differences for double support time were found between systems for the conditions of comfortable gait speed (mean –0.05 s and SD 0.07 s), slow gait speed (mean 0.28 s and SD 0.49 s), and toe walking (mean –0.17 s and SD 0.06 s). SEM and RCs were below the respective thresholds of 5 and 8% for all spatiotemporal gait parameters (≤ 2.4% and ≤ 6.3%, respectively), except for swing time (SEM range 3.9–9.4% and RC range 10.6–19.2%) and double support time (SEM range 9.3–40.4% and RC range 24.8–95.5%; Table II).
Excellent agreement for step length, step time, stance time, stride length, and stride time was found between the moving SGAS camera and the GAITRite® system with barefoot walking at comfortable speed (ICC ≥ 0.97 and lower limit of the 95% CIs ≥ 0.95; Table II). Paired t-tests revealed no differences exceeding the cut-off points of measurement error. Moderate agreement between systems was found for double support time and good agreement for swing time. SEM and RCs were below the respective thresholds of 5% and 8% for all spatiotemporal gait parameters (≤ 2.5% and ≤ 6.1%, respectively) except for double support time (SEM 10.2% and RC 25.6%).
Ten valid trials of footsteps were available for 25 subjects. Two footsteps were required to obtain excellent reliability scores (ICC > 0.90) for all 4 assessable spatiotemporal gait parameters for barefoot comfortable walking with the stationary SGAS setup (Table III). The CoV decreased gradually when averaging more footsteps. Four footsteps were required to reach a CoV below 10% for step length, step time, and stance time. The Bland-Altman plots showed no heteroscedasticity (Fig. 4). For double support time, 8 footsteps were required. For the shod walking condition, similar results were found. The sample sizes of the toe walking and slow gait speed conditions were too small, considering that there were fewer than 10 valid trials of footsteps per subject (sample sizes of 10 and 15 subjects, respectively).
The minimum number of footsteps needed for adequate reliability during comfortable barefoot walking by the moving SGAS camera in 30 subjects were 3 footsteps for step length, step time, and stance time and 7 footsteps for double support time.
Table III. Number of footstep repetitions for reliable spatiotemporal gait analysis system (SGAS) data for the barefoot comfortable gait speed condition by the stationary placed camera (n = 25)
Fig. 4. Bland-Altman plots of step length, step time, and stance time for 4 footsteps averaged with the stationary spatiotemporal gait analysis system (SGAS).
For assessment of the inter- and intra-rater reliability, 304–316 trials were used. Step length, step time, and stance time values had excellent agreement between the 3 observers (ICC ≥ 0.94 and lower limit of the 95% CIs ≥ 0.86). Inter-rater agreement on double support time was moderate (ICC 0.68 and 95% CI 0.48–0.79). Intra-rater reliability was excellent for step length, step time, and stance time (ICC ≥ 0.98 and lower limit of the 95% CIs ≥ 0.97), and good for double support time (ICC 0.84 and 95% CI 0.80–0.87).
This study found that the SGAS is a valid and reliable system to assess step length, step time, stance time, stride length, and stride time under different walking conditions. The stationary, as well as the moving, camera set-up can be used to determine these spatiotemporal gait parameters. However, validity could not be confirmed for double support time and swing time. A minimum of 4 footsteps was needed to obtain a reliable assessment of step length, step time, and stance time with the SGAS. Inter- and intra-rater reliability were confirmed for step length, step time, and stance time.
There is a need for low-cost and portable gait analysis technology in clinical settings. Such technology needs to be assessed for validity and reliability in assessing spatiotemporal gait parameters, such as in the current study using a 1-camera method. One other study using a 1-camera system examined the validity between this system and a reference 3-dimensional motion capture system (20). They found differences in accuracy between the 2 systems that were similar compared with the current study for the temporal parameters. However, they found larger differences between the system and the reference for the spatial parameters compared with our study, which may, among other possible explanations, be due to the choice of reference system. Results on reliability and measurement error were not reported in that study. Furthermore, they examined the validity for different gait speed conditions with the subjects wearing ankle socks, but not for the conditions of toe walking or shod walking. The Microsoft Kinect v2, which is a camera system extracting data from 3-dimensional skeletal modelling, has been shown to provide valid results for temporal parameters. Although results on accuracy for spatial parameters were inconsistent between studies (19, 21–24), one study showed an ICC of 0.76 for step length (95% CI –0.17 to 0.95) and an absolute and relative error of 10 cm (SD 5 cm) (21). Other low-cost alternatives using footswitches, accelerometers, gyroscopes, and inertial measurement units have been shown to be accurate in measuring temporal gait parameters, but are currently either unable or inaccurate to measure spatial parameters (25–30). Moreover, the advantage of a camera system over these methods is that video images of the person are obtained, which can be used for clinical assessment of gait pathology.
The SGAS is a feasible, easy-to-use measurement instrument for clinical practice and research purposes. In the current study, position and time assessment to calculate the spatiotemporal gait parameters from the SGAS user interface was a manual process. For experienced observers, position and time assessment for 10 trials in one walking condition took approximately 10–15 min. The observers noted that the video capture with time resolution of 0.02 s regularly missed the exact moment of initial contact or toe off, complicating the assessment. However, this did not compromise the reliability, since the results show that accurate data can be obtained with a 50 Hz sampling rate. The stationary camera set-up can be used in all settings, but is restricted by the field of view. In this study, the chosen field of view was 130 cm, to provide good spatial resolution for accuracy, but at the expense of being able to assess full strides. The use of a moving camera set-up solves this problem and, additionally, requires less effort from persons, as multiple steps are analysed in a single trial. A moving SGAS camera does, however, require a rail placed parallel to the walkway and a steady tripod on wheels. Recordings from the SGAS can be combined with other gait recordings (e.g. electromyography and force plate).
In this study, double support time and swing time could not be assessed in a valid and reliable way with the SGAS using the GAITRite® system as a reference. Whether this is a limitation of the SGAS or of the reference system is not fully clear, as no study on the measurement properties of the GAITRite® system has assessed how valid this system is in assessing double support time (15, 16, 32, 35–38), and only one study described swing time, but results on measurement error were not reported (16). In support of our findings, 2 other studies found moderate levels of agreement between the GAITRite® system and low-cost, portable systems for assessing double support time and swing time (26, 39). Perhaps the low time resolution of these systems (i.e. 50 Hz) could be an explanation for these findings, as double support and swing time are short events in the gait cycle. A camera with a higher sampling rate (e.g. 100 Hz) could be applied, but a disadvantage is that the size of the video data will substantially increase.
The current study has some limitations. The calculated minimum number of footsteps needed to achieve an adequate level of reliability for the SGAS data may not be generalizable to individuals with gait deviations. These individuals often show larger step variability and may show rotations in the transverse plane, such as foot inward rotation, which may lead to inaccuracies in measurements in the sagittal plane. Future research on this topic should include subjects with gait deviations and examine more than 10 trials of footsteps and strides, as recommended by other studies (16, 40). A second limitation concerned an error in the experimental set-up, where calibration of the SGAS was carried out on the floor and not on the GAITRite® carpet, which is 0.32 cm above the floor. This error has most likely influenced the differences found in the spatial parameters between the SGAS and the GAITRite® system (significant mean differences for step length of 0.06–1.24 cm). Finally, while data processing is not considered time-consuming, efficiency may be improved by automated processing. For example, in determining initial contact and toe off, which will also enhance accuracy and feasibility.
In conclusion, the SGAS is a valid and reliable system for assessing step length, step time, stance time, stride length, and stride time in different walking conditions and with both stationary and moving camera set-up. The validity of the SGAS for the assessment of double support time and swing time needs further investigation, preferably using a 3-dimensional gait analysis system as reference. Moreover, future research should validate the SGAS in subjects with gait deviations. A minimum of 4 footsteps is recommended for adequate reliability in each of the parameters tested, with a stationary camera.
The contribution of all subjects is gratefully acknowledged. The authors would like to thank G. E. A. van Bon, MSc, for support with the GAITRite® system, and M. E. Blankendaal, PT, who assisted in the data collection. We acknowledge E. J. P. Roek, M. W. Wojakowski, PT, W. Bout, MSc, B. N. Stevenson, PT, and R. L. van Halteren, PT, for their support with data analysis. In particular, we would like to thank H. G. van Bloemendaal, BSc, for making the software available as open source.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize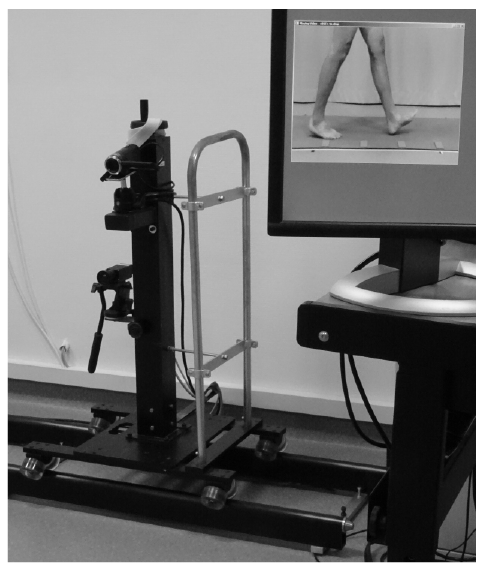 Click to show fullsize
Click to show fullsize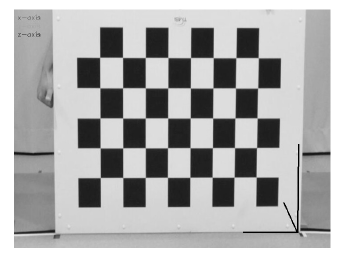 Click to show fullsize
Click to show fullsize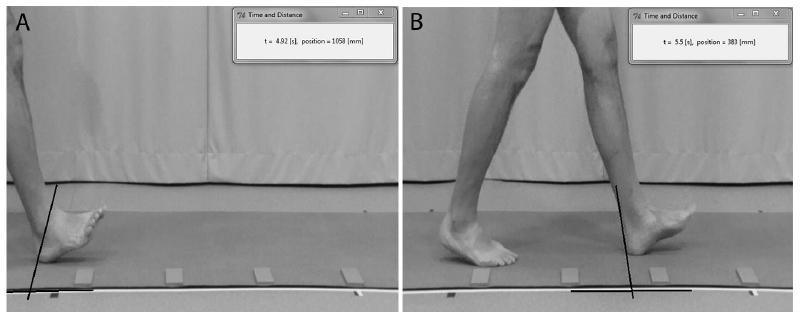 Click to show fullsize
Click to show fullsize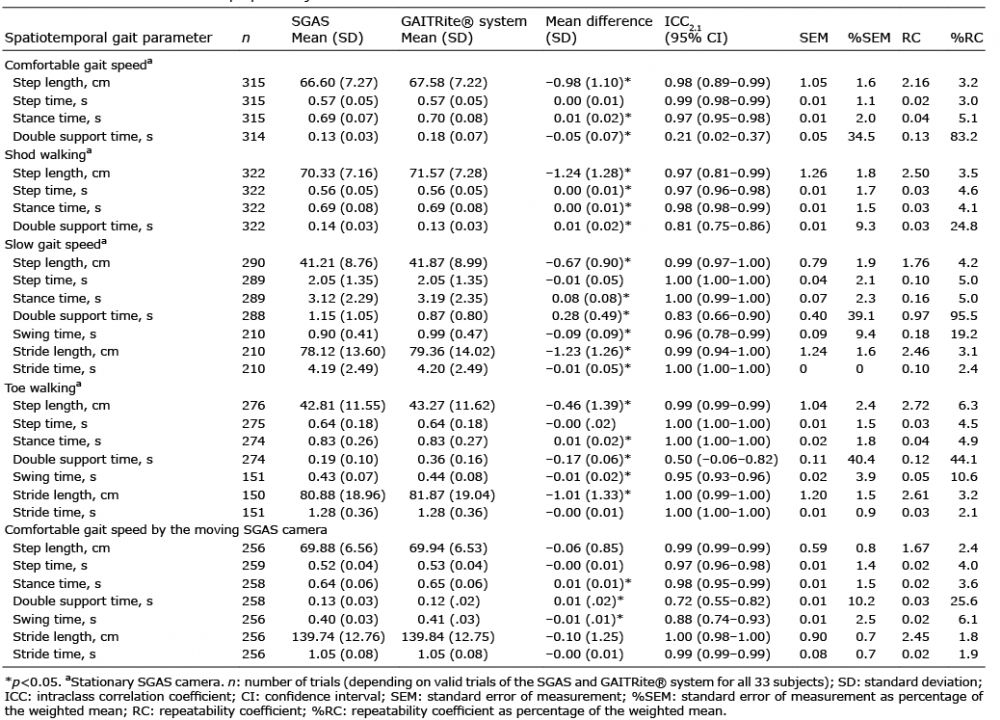 Click to show fullsize
Click to show fullsize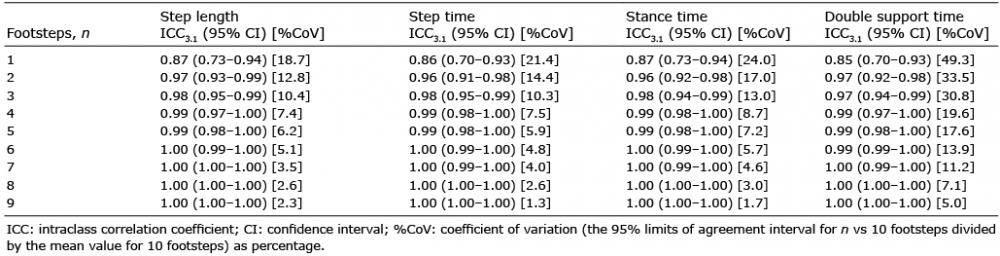 Click to show fullsize
Click to show fullsize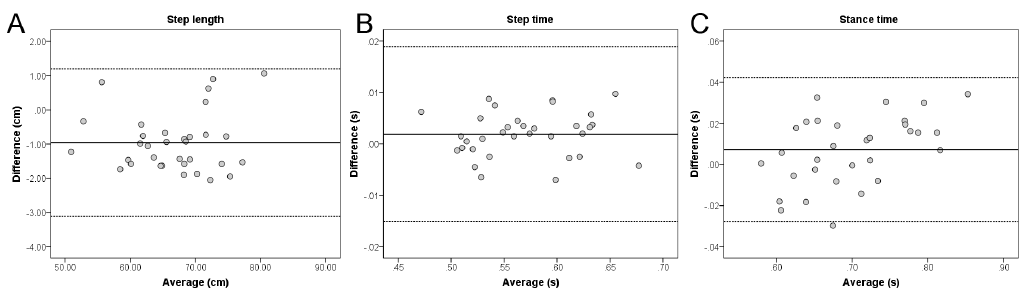 Click to show fullsize
Click to show fullsize